
Anatomy: The elbow is an inherently stable joint due to the congruity of the three bony articulations and the strong collateral ligaments. Additionally, when the joint is in extension (weight bearing position), the anconeus locks into the olecranon fossa providing even more stability. Elbow luxation requires significant soft tissue trauma with rupture/avulsion of the collateral ligament(s) and disruption of the flexors or extensor muscles originating on the epicondyles.
Elbow luxations are defined based on the displacement of the radius and ulna in relation to the humerus. The radius and ulna usually luxate laterally due to valgus forces during trauma, the presence of a prominent medial epicondylar ridge, and the fact that the lateral collateral ligament is stronger than medial collateral ligament.
Physical examination: Most dogs are non-weight bearing and hold the limb abducted, externally rotated and in slight flexion. Palpation of the elbow reveals pain, limited motion, crepitus, an indistinct lateral epicondyle, and displacement of the radius and olecranon laterally.
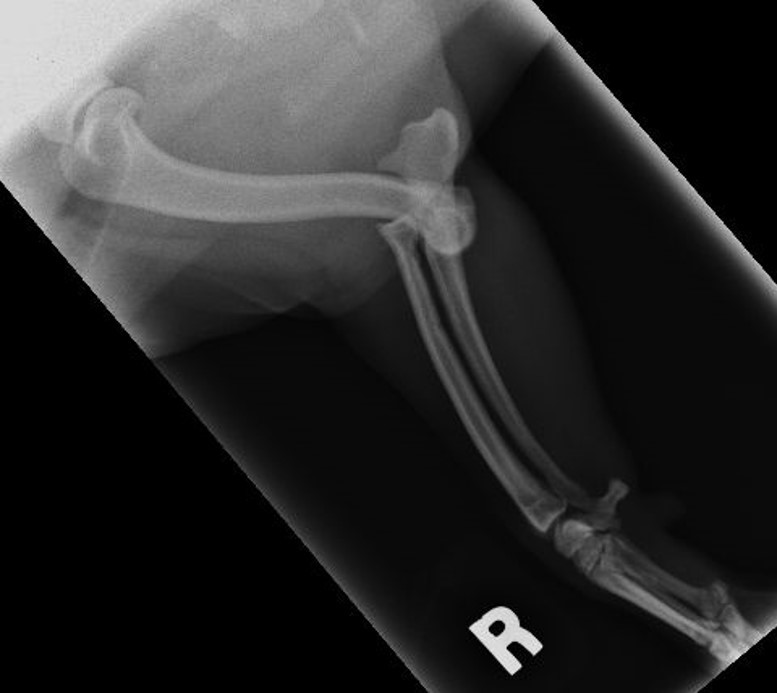
Diagnostics: Orthogonal radiographs should be performed. The anconeus may remain in the fossa but the radius and ulna are typically displaced laterally, cranially and proximally. It is important to look for any avulsion or articular fractures or evidence of dysplasia as these may preclude closed reduction.
Closed reduction: Most elbow luxations can be treated conservatively. General anesthesia is recommended to allow appropriate relaxation of the associated soft tissues. Apply traction to the limb for a few minutes prior to reduction. First, flex, abduct, and internally rotate the antebrachium to “hook” the anconeus into the  olecranon fossa. Then slowly extend the joint, maintaining internal rotation, and then place firm medial and distal pressure on the radial head. You may need to keep traction on the limb at the same time. You should feel a significant pop as the radial head reduces. Once reduced, confirm normal joint range of motion. Repeat radiographs to confirm appropriate reduction, then place a Spica splint.
olecranon fossa. Then slowly extend the joint, maintaining internal rotation, and then place firm medial and distal pressure on the radial head. You may need to keep traction on the limb at the same time. You should feel a significant pop as the radial head reduces. Once reduced, confirm normal joint range of motion. Repeat radiographs to confirm appropriate reduction, then place a Spica splint.
Open reduction: Indications for open reduction are: the presence of avulsion or articular fractures, soft tissue impingement in the joint preventing closed reduction, chronic luxation, and/or significant instability or re-luxation after closed reduction. Surgery typically involves reconstruction of one or sometimes both collateral ligaments. A Spica splint is placed post-op.
Post-reduction and post-op care: Pain management with an NSAID and gabapentin or tramadol as needed. The Spica splint is maintained for 3-6 weeks and exercise restrictions are recommended for 6 weeks. Once the splint is removed, rehabilitation (e.g. PROM) is recommend until limb use is normal.
Prognosis: Limb function depends on the degree of cartilage and soft tissue damage, the duration before repair, presence of persistent instability, and owner compliance. Since the joint is congruent, some degree of cartilage damage is expected when the joint luxates, so the owner should be warned about future joint OA. Prognosis is good-excellent if the luxation is treated early with closed reduction, the elbow remains stable after reduction, and rehabilitation is started early in the recovery process. Prognosis is less favorable if the luxation is chronic or if open reduction is required. Complications include recurrent luxation, bandage sores, decreased elbow ROM due to periarticular fibrosis, progressive elbow arthritis, and implant failure if open reduction is performed.